 The types of technology available have determined theories of brain function. When looking only at regional brain damage from trauma, theories arose of specific brain modules. Early imaging, also, furthered the notion of modules. But, in fact, the brain has many very active local hubs with massive interconnectivity including multisensory connections. There is no “center” of the brain. The “neuron doctrine” codified the incorrect notion that individual neurons explain brain function. More recent use of imaging with algorithms that subtract comparisons of active and placebo groups falsely correlates with module theories.
The types of technology available have determined theories of brain function. When looking only at regional brain damage from trauma, theories arose of specific brain modules. Early imaging, also, furthered the notion of modules. But, in fact, the brain has many very active local hubs with massive interconnectivity including multisensory connections. There is no “center” of the brain. The “neuron doctrine” codified the incorrect notion that individual neurons explain brain function. More recent use of imaging with algorithms that subtract comparisons of active and placebo groups falsely correlates with module theories.
 Now, the massive complexity of the brain has become apparent with constant simultaneous activity at many scales including genetic networks, proteins, lipids, neurons, synapses and wide spread circuits. Several previous posts described the limits of current neuroscience including our current inability to study individual neurons and to fully identify the changing circuits. A previous post described the almost insurmountable problems in projects attempting to understand the brain/mind by mapping the neuronal connections. This post will take a closer look at MRIs, which have become the fundamental tool for studies trying to correlate brain regions with circuits. There are, in fact, many limitations of MRIs for understanding behavior.
Now, the massive complexity of the brain has become apparent with constant simultaneous activity at many scales including genetic networks, proteins, lipids, neurons, synapses and wide spread circuits. Several previous posts described the limits of current neuroscience including our current inability to study individual neurons and to fully identify the changing circuits. A previous post described the almost insurmountable problems in projects attempting to understand the brain/mind by mapping the neuronal connections. This post will take a closer look at MRIs, which have become the fundamental tool for studies trying to correlate brain regions with circuits. There are, in fact, many limitations of MRIs for understanding behavior.
Brain Imaging Hype and Neuro Ethics
 There is much hype about how much is known about the brain. It makes for good news stories. It is prudent to quote from a major commentary from Nature magazine about correlating brain regions and circuits to human behavior.
There is much hype about how much is known about the brain. It makes for good news stories. It is prudent to quote from a major commentary from Nature magazine about correlating brain regions and circuits to human behavior.
“The general public might think that this goal has already been achieved; when they read that a behavior is associated with some part of the brain, they take that statement as an explanation. But most neuroscientists would agree that, with a few notable exceptions, the relationship between neural circuits and behavior has yet to be established.”
There are constant hyped claims in the media for the results of imaging studies. The public generally believes that individual brains can be studied with imaging to determine how and why behavior occurs. Even though these correlations are not proven, it is alarming to note that many scientists encourage these beliefs possibly to further their own funding.
The overhyping of imaging is not just an idle problem. It creates critical ethical problems for society when these false claims are used in courts. Other ethical problems include the possibility of enhancing the brain. This raises questions in academics that are similar to those of doping in sports. Could brain enhancement further society’s inequality?
Many Problems with Imaging
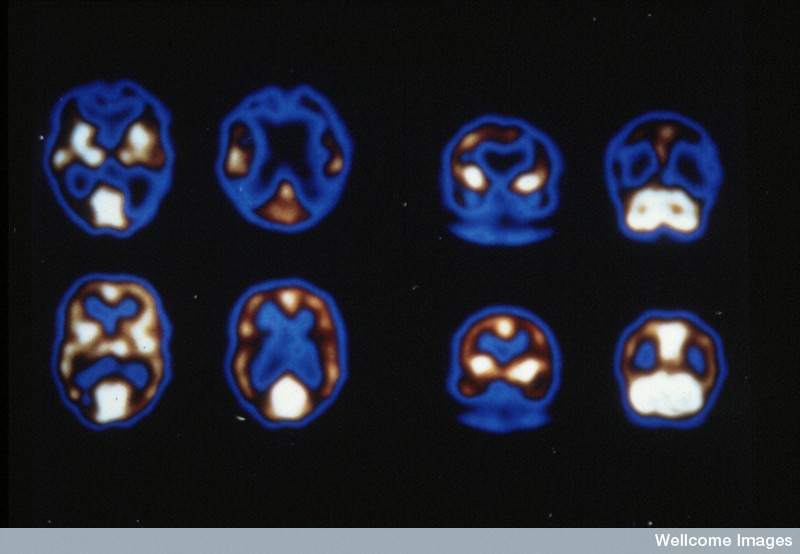
 Spatial resolution of the imaging technique is one problem when attempting to discover brain regions and circuits. PET scans have resolution of a centimeter, where each voxel of light is a huge brain region. For the MRI, each voxel of light represents the sum of blood flow in a region with about 80,000 neurons.
Spatial resolution of the imaging technique is one problem when attempting to discover brain regions and circuits. PET scans have resolution of a centimeter, where each voxel of light is a huge brain region. For the MRI, each voxel of light represents the sum of blood flow in a region with about 80,000 neurons.
Even when activity at different scales appears to correlate with behaviors, there is no way to determine causality. Other factors might be causing the effects indirectly or through rapid circuits that are not observable. Genetic studies that attempt to correlate brain regions, MRI and cognitive functions have not been successful, either.
There are many different types of problems in attempting to correlate brain regions and behavior. Brain stimulation is one way to look at specific regions and brain function. These studies are greatly limited by the rare situation where neurological treatment requires brain implantations. Transcranial stimulation, which is not invasive, occurs over too large an area to be precise.
 A major problem is that it is not clear what scale to study-organelles, synapses, neurons, glia, immune cells, neuronal hubs with local and long distance connectivity, brain regions, whole brain, whole body and interpersonal levels all at once. Also, Individual brains change so much through neuroplasticity that, in fact, each has different circuits at microscale.
A major problem is that it is not clear what scale to study-organelles, synapses, neurons, glia, immune cells, neuronal hubs with local and long distance connectivity, brain regions, whole brain, whole body and interpersonal levels all at once. Also, Individual brains change so much through neuroplasticity that, in fact, each has different circuits at microscale.
Glia create much more complexity. Even larger than the neuronal network is the calcium based astrocyte network, which produces, maintains and prunes the neuronal synapses. The oligodendrocytes create a unique myelin code. Microglia are part of the wireless immune brain, which responds to both infections and mental events, working with astrocytes to maintain and prune synapses.
Problems with MRI
 The major tool in current neuroscience is MRI. Previous posts have describes a number of specific issues with MRI in determining cognitive function. This post has more details. A list of the previous issues are listed here:
The major tool in current neuroscience is MRI. Previous posts have describes a number of specific issues with MRI in determining cognitive function. This post has more details. A list of the previous issues are listed here:
- A widespread experimental assumption in most MRI studies is not certain. This assumption compares an “active” group and control by adding activity to the control’s activity, rather than subtracting.
- Each dot of light on fMRI (voxel) measures average blood flow activity in a region of 80,000 neurons and 4 million synapses over a second.
- Blood flow is determined by astrocytes not neuronal activity.
- By the time the blood flow is measured over one second, activity has occurred in milliseconds all over the brain
- Large MRI study used 500 repetitions and found the brain regions chosen in most studies wouldn’t be valid with the small number of repetitions used in most studies. Studies with small “n” find the strongest region. More detailed study showed many small regions all over the brain. The time chosen for the “strongest signal” is arbitrary and many small regions fire before and after time.
- Each test was different because of learning effects from one trial to the next
- The new diffusion MRI techniques measure water, possibly inside and outside the membrane. It is not, yet, clear what this measurement means.
- Brain wave studies show rolling effects all over brain not one region. The “n” of almost all neuroscience studies are too small to find statistical significance Changing neuroplasticity produces new synapses and prunes them every day
MRIs Try to Measure Behavior
 Even though MRIs are ubiquitous in medicine and neuroscience, they were only developed in this generation. While, the physics was discovered in the 1930s, the first patents were in the seventies. MRIs were introduced into medicine in the 1980s. By 2002 there were 20,000 in medical practice with 60 million procedures.
Even though MRIs are ubiquitous in medicine and neuroscience, they were only developed in this generation. While, the physics was discovered in the 1930s, the first patents were in the seventies. MRIs were introduced into medicine in the 1980s. By 2002 there were 20,000 in medical practice with 60 million procedures.
The major MRI technique measures blood oxygen level dependence (BOLD), which is based on blood flow in a region. Astrocytes control the blood flow (see post on astrocytes) and the astrocyte network (larger than neuronal network) interacts with every part of the neuronal circuits. Astrocytes are involved in producing, maintaining and pruning all synapses.
The exact relationship of neuronal activity and astrocyte controlled blood flow is not certain. BOLD does correlate in many cases with the amount of neuronal activity and the local field gradient. But, this is not always the case. In fact, it can be completely different.
The blood flow changes occur after the neuronal activity (stimulated by it) and are related to post synaptic activity, not axon spikes. Blood flow can, also, be related to sub threshold electricity.
Representation of Behavior with MRI
 Brain mapping charts MRI activity in a particular region and attempts to correlate this with a mental event. Studies of this type show regions that might be activated with particular states, but not how mental events occur. There are several new techniques developed to try to capture more information.
Brain mapping charts MRI activity in a particular region and attempts to correlate this with a mental event. Studies of this type show regions that might be activated with particular states, but not how mental events occur. There are several new techniques developed to try to capture more information.
MRIs are not photographs as many people incorrectly think. They use mathematical algorithms to combine many “slices” of the brain into a larger coherent image. The standard algorithm has been used for many years with a large amount of normative data. In order to try to get more information from the same data, new mathematical techniques are being developed without this normative experience.
Multi voxel pattern analysis (MVPA)
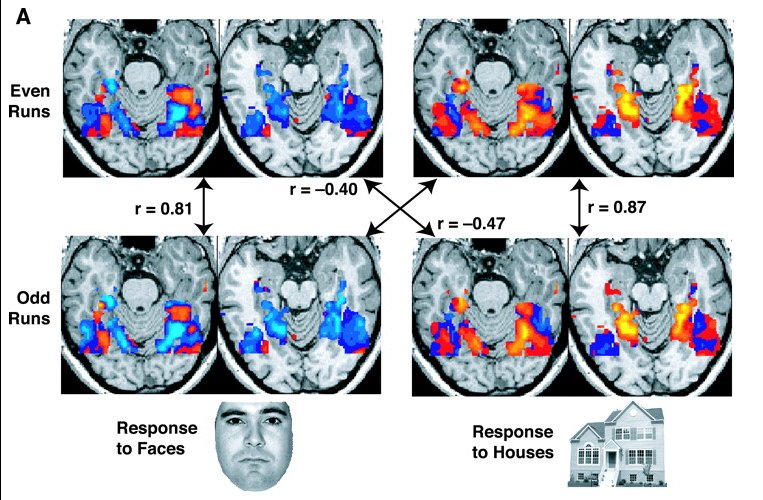 This technique tries to relate psychological mental events with machine learning. It is used with specific mental events for an individual person. Research with this technique includes using BOLD patterns to describe visual material such as faces. It has, also, been used to find the meanings of specific words with MRI patterns. One use of this technique is called voxel-wise modeling, which estimates words and scenes in movies being watched.
This technique tries to relate psychological mental events with machine learning. It is used with specific mental events for an individual person. Research with this technique includes using BOLD patterns to describe visual material such as faces. It has, also, been used to find the meanings of specific words with MRI patterns. One use of this technique is called voxel-wise modeling, which estimates words and scenes in movies being watched.
The technique has demonstrated that attention alters what some stimuli represent in different regions of the cortex. It, also, demonstrates what is not altered. One particular study showed that when two memories are competing for space in active conscious (working) memory they are not remembered well.
The difference between MVPA and regular MRI is that with MVPA each voxel is examined in relation to each other with advanced mathematical formulas. An example may include twenty voxels each studied compared to the others. The regular MRI measures the averages from the categories studied. MVPA uses a complex mathematical algorithm to study multi dimensional relationships between all of the voxels in the study. The mathematics uses twenty dimensional space for twenty voxels, which is then projected onto a two dimensional picture. This is complex, abstract mathematics, with uncertain results related to mental events.
Representational Similarity Analysis (RSA)
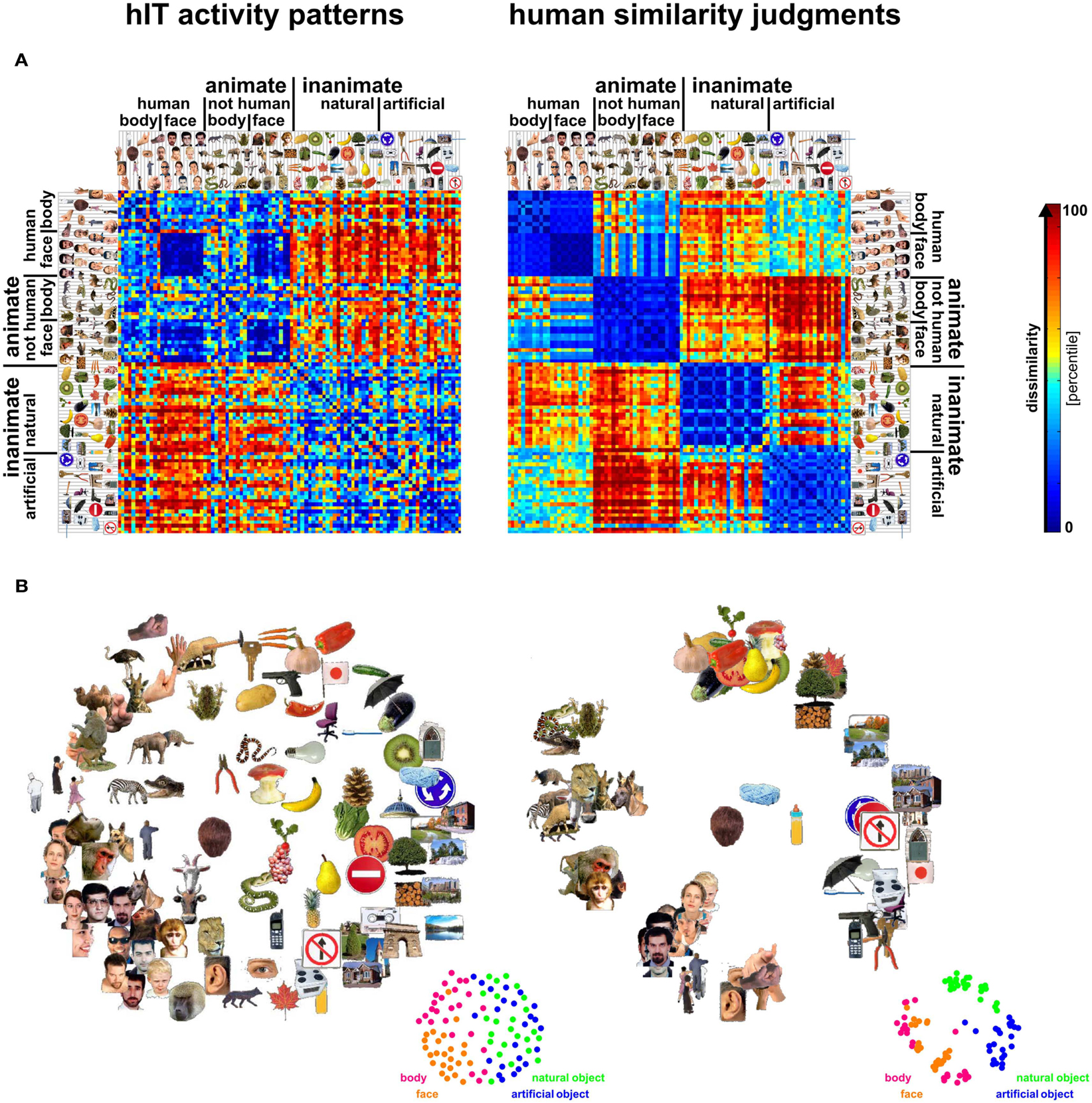 A second technique representational similarity analysis (RSA) attempts to correlate how specific sensory inputs make patterns that are related. It tries to find how we mentally know how objects are related and what patterns this mental understanding produces. It can be used in situations to find out what is learned.
A second technique representational similarity analysis (RSA) attempts to correlate how specific sensory inputs make patterns that are related. It tries to find how we mentally know how objects are related and what patterns this mental understanding produces. It can be used in situations to find out what is learned.
RSA is used to understand the many types of mental events that occur in wide circuits throughout the brain, such as pain. RSA uses a different mathematical algorithm correlating all items and finding which have high or low correlations.
Research has identified limits of both of these mathematical approaches. Of particular importance, is the fact that they do not determine what causes mental events. In fact, these new mathematical models need many years of validation.
MRI and Computer Models
 Attempts are made to use computers to model neuronal decision making in experiments related to brain function. Previous posts have shown how difficult it is to decipher how neurons make decisions when to fire (Searching for the Neural Code). These models of decision making are then correlated with computer models of MRI data. There are many assumptions made in this results and the results are general, but suggestive.
Attempts are made to use computers to model neuronal decision making in experiments related to brain function. Previous posts have shown how difficult it is to decipher how neurons make decisions when to fire (Searching for the Neural Code). These models of decision making are then correlated with computer models of MRI data. There are many assumptions made in this results and the results are general, but suggestive.
An example involves animal behavioral experiments using reinforcement and rewards. It is known that dopamine in the striatum is one signal of reward. A previous post described how complex the dopamine system is. Computer models connected with MRIs have shown that there are multiple different systems that remain extremely complex and not well understood.
Another computer model connected with MRIs is the new memory research on pattern completion and separation described in previous posts. These studies attempt to correlate specific MRI signals to groups of neurons related to this activity.
Imaging and Genetic Networks
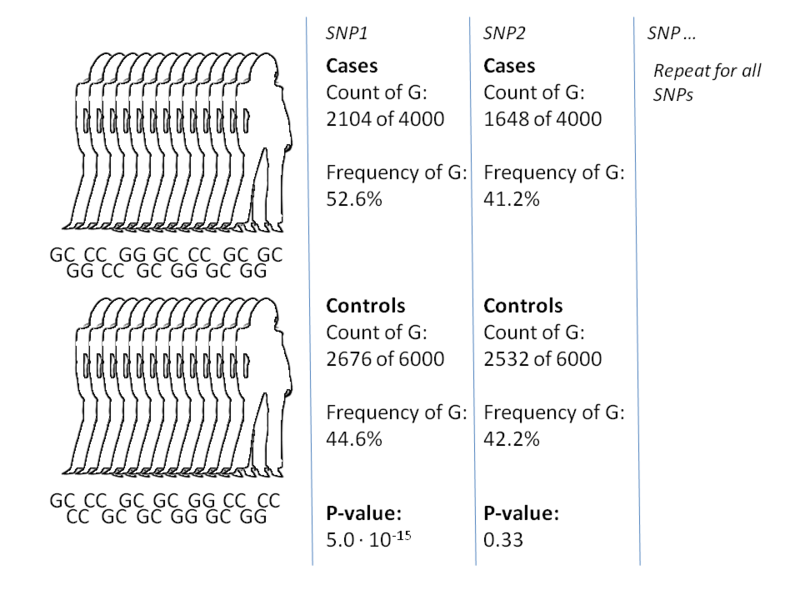
There is some evidence that BOLD responses are similar for those genetically related. Some genes have been correlated with BOLD signals as well. But, large studies have not found useful correlations. A very large recent study of genome wide association studies (GWAS) showed that previous smaller studies were incorrect. The correlations from these previous studies correlating brain volumes with genes were not at all found in the large GWAS studies.
There has been a lot written about specific genes and cognition such as COMT gene and memory. But, the studies comparing these genes with brain imaging show no correlation. It appears that the correlations were from small studies (small n) and publication bias-publishing small studies that do not have enough subjects to substantiate the claims.
To compare GWAS genetic data with brain structures from MRIs requires tens of thousands of subjects, which is currently not possible.
Default Mode Network
Previous posts on meditation have described the new major research on brain activity during the resting, not focused, relaxed, daydreaming state. In fact, many different networks are being found that appear to be related to a sense of who we think we are. These networks are being deciphered by analyzing complex signals that occur in this resting state.
The major work up until recently has been with activity between the anterior and posterior midline regions, the lateral temporo-parietal cortex and the medial temporal lobe-known as the default mode network (DMN). This system is not at all active during any focused activity and becomes very active at rest. A similar system appears in mice and in other primates. These regions are damaged during Alzheimer’s dementia.
Recent research attempts to correlate MRI data about the default mode network circuits and the activity that occurs during specific mental focus during activities. Computer models attempt to correlate which voxels are used in DMN and in the specific activity to see if there are similar patterns. These studies used data from a large number of different people to find some similarities. Also, studies of individual brain readings showed potential correlations.
But, all of these studies have many problems of interpretation and are quite theoretical. It is not possible to use them with individuals. Problems of interpretation include whether sleep intrudes on the study of resting state and what position and head motion are due to the activity.
MRI in Psychiatric Diagnosis and Treatment
 Animal models of psychiatric disorders are all inexact and do not describe the human disorder accurately. Currently, there are no accurate biological tools to diagnose psychiatric illness. Diagnoses are made by constellations of specific behaviors that seem to have clinical relevance through clinical studies. Despite generations of work and thousands of studies, currently, psychiatric diagnosis is made from syndromes that include specific set of symptoms, not biological data. There have been no adequate biological descriptions.
Animal models of psychiatric disorders are all inexact and do not describe the human disorder accurately. Currently, there are no accurate biological tools to diagnose psychiatric illness. Diagnoses are made by constellations of specific behaviors that seem to have clinical relevance through clinical studies. Despite generations of work and thousands of studies, currently, psychiatric diagnosis is made from syndromes that include specific set of symptoms, not biological data. There have been no adequate biological descriptions.
A new type of diagnostic system is being considered that is based on measurable impairments in brain circuits or systems. While these systems are vague, there is some chance of correlating them eventually with brain circuits and levels of activity. Data could include MRI data, molecular biomarkers and descriptions of circuits such as the fear or reward systems. Currently, attempts to define diagnoses in this way do not correlate with the existing clinical symptom categories or definitions.
One specific example of this type of new diagnostic approach involves depression. It is possible that depression is relation to the specific region of the cingulate cortex (the sub-genual anterior cingulate cortex). This research attempts to treat the mood disorder with specific electrical stimulation of this region through deep brain stimulation with implanted brain electrodes and use of MRIs. Other research uses brain stimulation from the surface (without invasive electrodes) in the lateral pre frontal region. This latter treatment has been approved by the FDA with transcranial magnetic stimulation (TMS) when the depression is extremely severe and does not respond to any conventional treatment. Another use of imaging for treatment is using it as feedback to individuals to study treatment of pain and depression.
These attempts have not been completely successful and there is no consensus that they can be used for diagnosis and treatment. In fact, a recent large study showed that using structural brain changes in specific regions are not currently useful to diagnose psychiatric illness. Attempts have been made to correlate specific gene activity in regions with other data from imaging to attempt to identify molecular circuits related to diagnoses. These are ongoing and have no definite findings.
New research includes trying to use the new science of opto-genetics and combining it with MRI. Techniques now exist to use light switches to alter neuronal behavior in animals. One day these light switches might help identify circuits in live human brains without implanting electrodes. This could replace invasive stimulation. This could lead to the development of a new optical MRI.
Neurological Illness
 There are ongoing attempts to correlate imaging findings in the quest to diagnose and treat Alzheimer and other dementias. Some think that people with dementia can be predicted before the onset of clinical symptoms using these techniques. However, this has not yet been proven and many claims are made prematurely in the media to attract funding. In fact, large studies assume that they can predict who will get dementia for drug trials, even though this is not proven.
There are ongoing attempts to correlate imaging findings in the quest to diagnose and treat Alzheimer and other dementias. Some think that people with dementia can be predicted before the onset of clinical symptoms using these techniques. However, this has not yet been proven and many claims are made prematurely in the media to attract funding. In fact, large studies assume that they can predict who will get dementia for drug trials, even though this is not proven.
The problem in the studies of this type is the assumption that these early findings represent the early disease. Some look for regional brain atrophy patterns and some look for tagged molecules, such as amyloid. Then treatments are applied to avoid the onset. But, it is not really clear whether pre clinical evaluation is accurate. For example, for a long time there has been a research assumption that finding many amyloid plaques in the brain predicts Alzheimer’s. But, more recent studies find some people have substantial amyloid without Alzheimer’s, as well as the opposite-some people with dementia may have less amyloid. It is possible that it is the tau tangles are more relevant. Very recently the processes that create tau tangles and amyloid plaques have been connected in experiments (see post).
One area where imaging is increasingly helpful is in investigating “vegetative states,” that is, patients who cannot move or respond because of paralysis. Some of these people are aware, but cannot tell us anything. Recent research can allow some patients previously deemed “brain dead” to use computer cursors to communicate. These “locked in” states are now an area of intense research.
Predicting With MRIs
 Can imaging help predict behavior? Extensive research for marketing uses focus groups and now increasingly brain-imaging patterns. Neuro-marketing includes some scientific research, but mostly commercial efforts.
Can imaging help predict behavior? Extensive research for marketing uses focus groups and now increasingly brain-imaging patterns. Neuro-marketing includes some scientific research, but mostly commercial efforts.
In one scientific study people listened to new songs and then gave their impressions. Brain scans of their reward brain centers were analyzed, as well. Years later, it appears that the MRI brain activity better predicted interest than the subjective report. More people with MRI activity eventually bought these particular songs, than those with the subjective positive report.
This same finding occurred with anti smoking and healthy food programs. It is possible that imaging can predict better academic performance, as well. All of these studies have a major limitation related to the small sample sizes with similar types of subjects.
Imaging For Courts

A very critical type of research involves neuroscience used in courts to decide competence to stand trial and responsibility for a crime. It is important to realize that imaging doesn’t prove causality and that most legal claims for MRI are completely unproven. Often this is overlooked in the court hearings. It is a confusing area because all actions are related to brain activity and a finding of activity doesn’t imply causation or responsibility. Does finding a tumor mean that it caused the person to commit the crime? Recently, in one famous Supreme Court case, neuroscience was used to change life imprisonment rules for children who commit crimes. Its not clear that the neuroscience should have been used.
The biggest problem of using imaging data in a courtroom is that all of the imaging conclusions are general results in groups of people and do not relate to individuals. The individual information is extrapolated, not proven. Many have used “lie detectors” in legal proceedings, but these are being shown to be questionable for individuals and can be consciously fooled.
One day, imaging measurements might be able to define the degree of pain an individual has. But, currently it is too complex. Therefore, imaging is not able to distinguish whether pain exists or not when considering malingering.
Future Devices
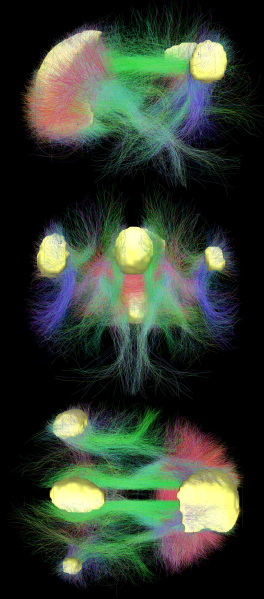
 With all of the problems and inadequacies of MRIs, the Brain Project is attempting to develop totally new ways of imaging brain function. One is optical coherence tomography. Diffusion MRI imaging is being developed, but has many problems as well, including an inability to track long circuits.
With all of the problems and inadequacies of MRIs, the Brain Project is attempting to develop totally new ways of imaging brain function. One is optical coherence tomography. Diffusion MRI imaging is being developed, but has many problems as well, including an inability to track long circuits.
Regular MRIs use one brain slice at a time to make pictures. New types use eight images at once. Also, they use much stronger magnets to get better resolution. But, this can create new types of “noise” in the pictures. As the details grow, so do the mathematical assumptions and algorithms, which may not be correct. Diffusion technology views water molecules in more directions-from 64 to hundreds-that allows a view of smaller bundles. But, this has inherent limitations.
Also, there is increasing evidence that many of the MRI studies are not reproducible. These many problems have been listed in other posts-complex dimensional analysis with unproven assumptions, numerous analytic techniques that have not been compared and very small number of subjects that do not allow for statistical proof.
Limitations of MRIs for Understanding Behavior
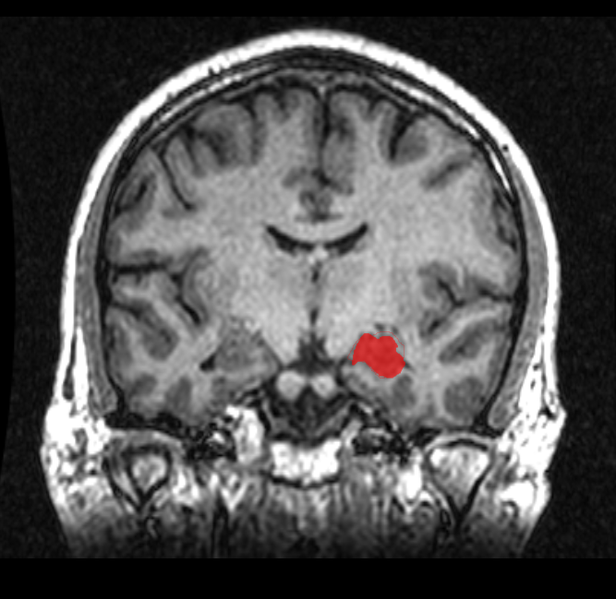
 While the attractive pictures of brain imaging are exciting and interesting, it has to be understood that these images are, in fact, computer models built upon algorithms that may or may not relate to reality. They are not photographs. There are many other problems listed in previous posts with research using imaging.
While the attractive pictures of brain imaging are exciting and interesting, it has to be understood that these images are, in fact, computer models built upon algorithms that may or may not relate to reality. They are not photographs. There are many other problems listed in previous posts with research using imaging.
Perhaps the biggest problem with MRIs is that the resolution of MRIs (the dot of light on the screen) is the average of blood flow over a second in a region of 80,00 neurons. It is now understood that brain activity occurs in milliseconds. A neuron can be part of one large circuit across much of the brain in one millisecond and suddenly part of a different circuit through its 10,000 different connections.
There has been no progress in finding a center for awareness and consciousness in the brain. Most mental events produce activity throughout the entire brain. There is no module or region to be found in an MRI that is the subjective experience, which is the substance of our lives. This subjective experience is very complete, binding together all kinds of sensory data, concepts, thoughts of past and future, feelings, associations and memories.
The current research is more consistent with mind existing as an integral aspect of nature, like energy and matter, interacting with the constantly active and evolving brain.